


This poster highlighting an integrated tele-antimicrobial stewardship clinical decision support system implementation was originally presented at IDWeek 2021, held virtually Sept. 29 – Oct. 3, 2021.
Sui Kwong Li, M.D.1,2; Erin K. McCreary, PharmD1,2; Tina Khadem, PharmD1,2; Nancy Zimmerman, RN, BSN2, Sarah Burgdorf, M.D., Ph.D.1,2, Nupur Gupta, DO MPH1,2, Kate Gass, BSN3, Gary S. Fisher, PharmD3, James W. Backstrom, M.D.3, Robin L. Portman, PharmD3; Sara Schwarz, PharmD3; Kimberly Schultz, RPh3, Jenessa Heller, PharmD3, Kris Bearer, RPh3, Jayne Schreckengost, RPh3, Jennifer Prazenica, RPh3, John W. Mellors, M.D.1,2; Rima C. Abdel-Massih, M.D.1,2; J. Ryan Bariola, M.D.1,2
1. Division of Infectious Diseases, UPMC 2. Infectious Disease Connect, Pittsburgh, PA USA 3. 3 Armstrong County Memorial Hospital, Kittanning, PA
Conclusions
- Tele-Antimicrobial Stewardship Program (TASP) in a rural community hospital resulted in a high percentage of accepted stewardship interventions and lower antimicrobial usage.
- Success is dependent on robust educational efforts, establishing strong relationships with local providers, and involvement of key stakeholders.
- Lack of dedicated stewardship time for local pharmacists is a very significant barrier to TASP success.
Objective
- Small hospitals in the US may lack access to infectious diseases (ID) expertise despite similar rates of antimicrobial use and drug-resistant bacteria as larger hospitals.
- A tele-antimicrobial stewardship program (TASP) is a force multiplier, expanding access to specialty care, training, and guidance on appropriate resource utilization.
- Data on the impact of TASPs in community or rural inpatient settings is limited.
Background
- Small hospitals in the US may lack access to infectious diseases (ID) expertise despite similar rates of antimicrobial use and drug-resistant bacteria as larger hospitals.
- A tele-antimicrobial stewardship program (TASP) is a force multiplier, expanding access to specialty care, training, and guidance on appropriate resource utilization.
- Data on the impact of TASPs in community or rural inpatient settings is limited.
Methods
- We established a TASP at a 160-bed hospital in Armstrong County, PA (population 65,000) in September 2020.
- Tele-ID consult services were already being used as of April 2020.
- A non-local ID pharmacist or ID physician with access to the local electronic medical record performed prospective audits and provided feedback with 1 local pharmacist on a 30-minute video conference daily.
- At TASP implementation, all patients receiving intravenous (IV) fluoroquinolones, metronidazole, and azithromycin were reviewed.
- Figure l shows the timeline of TASP implementation.
Results
- From September 2020 to August 2021, 406/519 (78%) stewardship opportunities were accepted (Figure 2).
- Monthly antimicrobial use declined on average from 673 DOT/1000 PD to 638 DOT/1000 PD (Figure 3).
- Daily calls involved ~5 patient reviews though ~20% were cancelled on weekdays due to staffing shortages.
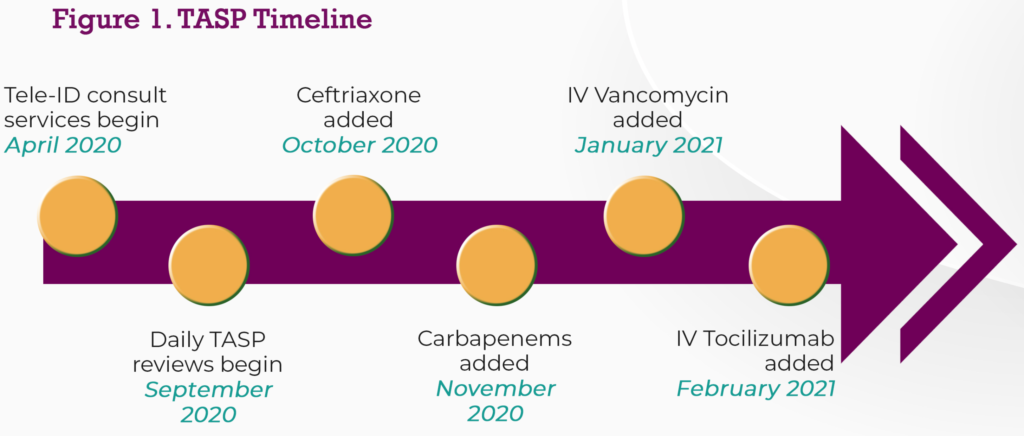
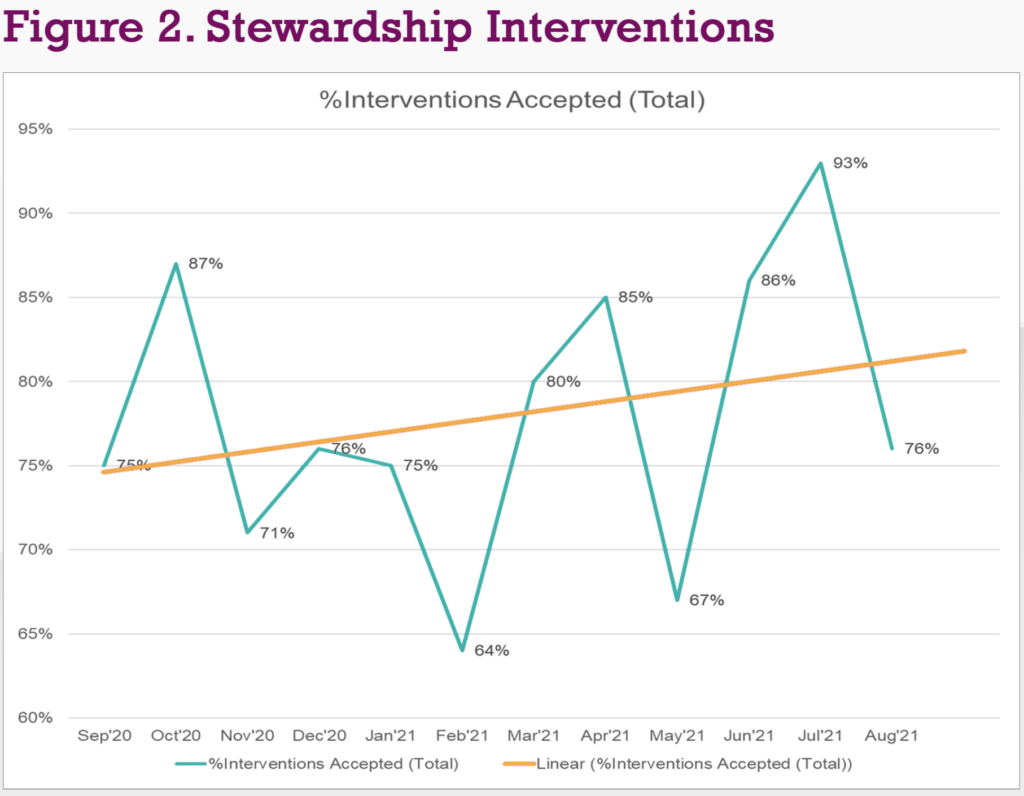
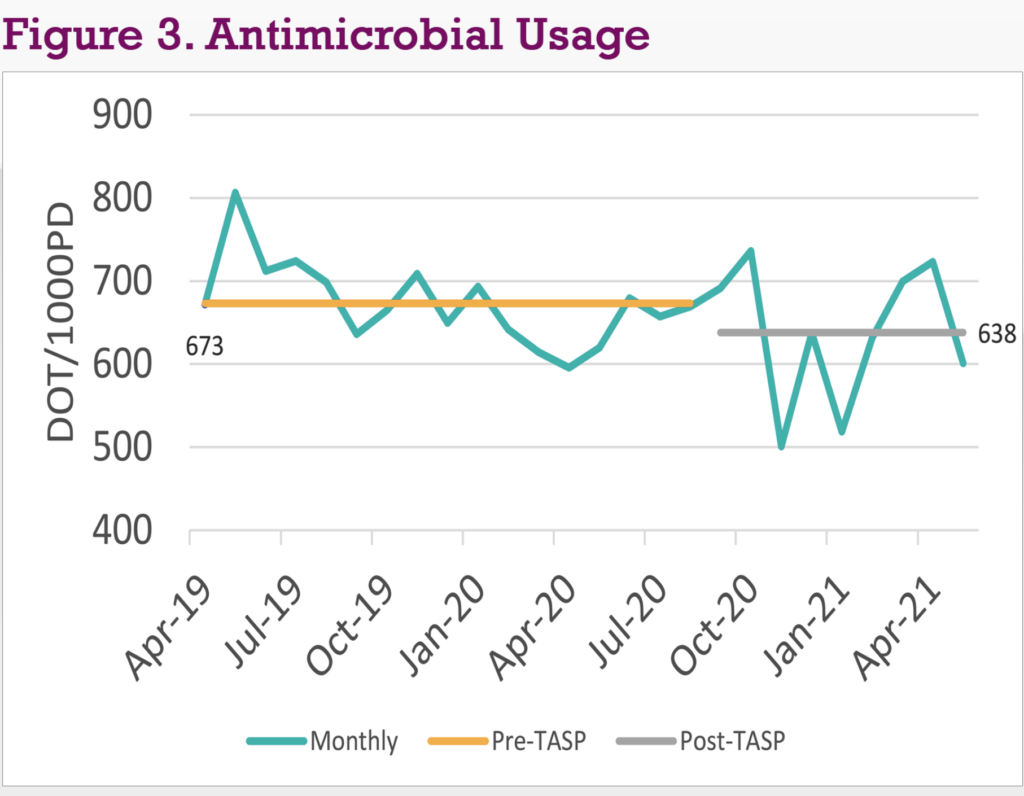
Table 1 TASP Accomplishments
| Patient Care | Guidelines | Microbiology Lab | Policies | Education |
|---|---|---|---|---|
| Available for patient-related questions via email outside of daily TASP call | Empiric antimicrobials for common infections | Enhanced culture results display to providers in electronic health record for improved readability | Indications for use on electronic antibiotic orders | Introduction to stewardship webinar |
| Coaching on conducting through beta-lactam allergy history | COVID-19 | Added clinician comments to culture and laboratory test results | Surgical prophylaxis | Monthly stewardship pearl newsletter |
| Stewardship intervention form | CAP | Updated AST panels and reporting rules to align with current breakpoints | Aminoglycoside dosing | Tocilizumab weinar |
| Patient monitoring form | HAP/VAP | Revised antibiotic reporting rules for Enterococcus spp. isolated in urine cultures | Renal dosing | COVID-19 monthly updates and webinars |
| Prospective audit with feedback M-F | Procalcitonin | Revised cascade reporting rules | MDRO and isolation | |
| IV to PO conversion | Updated local antiiogram | Vancomycin dosing in dialysis |
You might also like…

ID Connect Named to Becker’s Health IT “Telehealth Companies to Know” List for the Third Year in a Row

Infectious Disease Connect Strengthens Clinical, Operational, and Growth Leadership Amid Continued Expansion

The Hidden Risks of Limited Infectious Diseases Coverage