
Infectious disease (ID) medicine has a numbers problem. There are not enough providers to adequately meet the current level of patient demands, nor enough trainees in the pipeline to rectify the situation. It’s easy to intuit the many consequences: longer waits for appointments, patients having to travel farther for specialty care, delays in care, or fewer chances to ensure optimal health and disease-state management. The list can be added to, but the end products of the equation are the same – suboptimal patient care, provider burnout, and increased costs for hospitals and facilities.
Consider that more than 80% of counties1 in the United States do not have access to a single ID specialist. Also, consider that in the 2022 National Resident Matching Program (NRMP), infectious disease fellowships nationally had a paltry 56% match rate2 for adult ID training programs and 49% for pediatric ID training programs, while most other specialties, like cardiovascular disease, clinical gastroenterology, and interventional pulmonology filled all or nearly all their residency slots2.

Not enough trainees and not enough established providers, yet the patient need is still there – especially given the continually emerging and evolving challenges hospitals face in dealing with the diversity of ID, including:


- Emerging – and re-emerging – infectious diseases. (E.g., monkeypox, measles, RSV, COVID-19, etc.)
- Seasonal influenza
- New and stronger antimicrobial resistant bacteria due to poor use or patient adherence, over prescription, rampant use of antibiotics in livestock, and few novel agents in development
- Challenges in administering and maintaining robust antimicrobial stewardship programs
What happens when the average person needs ID care and they are in an area or facility with limited options? They must travel long distances to major cities or academic medical centers that have more robust ID programs. or they get transferred from one hospital to another, again often out of their local community. Patient care suffers and there can be harm. It’s not an ideal situation for patients or physicians.
So, what are some solutions that can make immediate and substantial change? At the top of the list: Telemedicine.
Why ID Care and Telemedicine Are Perfect Partners
Telemedicine is rapidly becoming mainstream for many medical disciplines, embraced by both providers and patients for the tremendous benefits it provides. This is equally true for the field of infectious disease medicine. Telemedicine is an apt partner for ID care delivery because tele- ID practitioners can more easily manage their consult caseloads across multiple facilities while key microbiology and other lab results are processed. As a medical specialty, ID experts have more consistency in their care protocols. Effective ID consults can happen in a doctor-to-doctor phone call. When more research is needed, asynchronous ID consults can easily be supported by having an ID expert leave detailed notes in a patient’s electronic health record for their general physician to act upon the next day. When tele-ID experts need to “see” patients, nurses and other advanced practice practitioners can easily do needed hands-on examinations under the tele-direction of an ID expert.
Since tele-ID was first introduced at UPMC in 2013, the hospital system and its ID experts have had a rare opportunity to look at the differences in cost-savings, access to care, scalability of services, and the impact of supporting technologies between tele-ID and in-person ID consults in their inpatient facilities.

Infectious Disease Connect Lays Out Rationale for ID Telemedicine with Recently Released Study Findings

In a recently published study3 in the academic journal Open Forum Infectious Diseases, ID researchers, clinicians, and leaders of Infectious Disease Connect detail findings from a retrospective analysis of three community hospitals (in largely rural areas/counties in northwestern Pennsylvania) in the UPMC system that converted from an in-person infectious disease care model to one based solely on ID telemedicine services provided by Infectious Disease Connect’s clinicians.
The study analyzed outcomes for ID patients at the three hospitals during a six-month period in which in-person ID care was available, and the immediate six-month period when ID telemedicine replaced the in-person care model. The study examined consultation rates between the two paradigms, hospital length of stay, transfers to tertiary care centers for ID patient care, percentage of discharges to home, 30-day readmission rates, and mortalities.
Data for the in-person care cohort was pulled from January 1 – June 20, 2018, while the ID-telemedicine data was pulled from patient records between July 1, 2018, and December 31, 2018. There was a total of 251 cases in the in-person care cohort, and 391 in the ID-telemedicine group. The combined in person and tele cases involved more than 30 types of infectious diseases with abscess, asymptomatic bacteriuria, Clostridioides difficile, osteomyelitis, prosthetic joint infection, and septic arthritis being the most common diagnoses.
Outcomes across all measures between the groups were equivalent, with trends toward lower rates of 30-day readmissions, transfers, and length of stay in the ID-telemedicine cohort. Mortality within 30-days of discharge was also equivalent.
While this study used a small cohort from only three hospitals, it represents the first solid data comparing outcomes between patients who received ID care through a telemedicine-based approach versus an in-person specialist handling care on-site.
What Patients and Healthcare Providers are Saying About Telemedicine
The success of any ID telemedicine approach ultimately comes down to how patients react and accept receiving care or communications through tele-consults and how providers themselves navigate the telemedicine systems. For both patients and providers, ease of use, consistency of communications, and robustness of clinical information drive the acceptance of this care model.
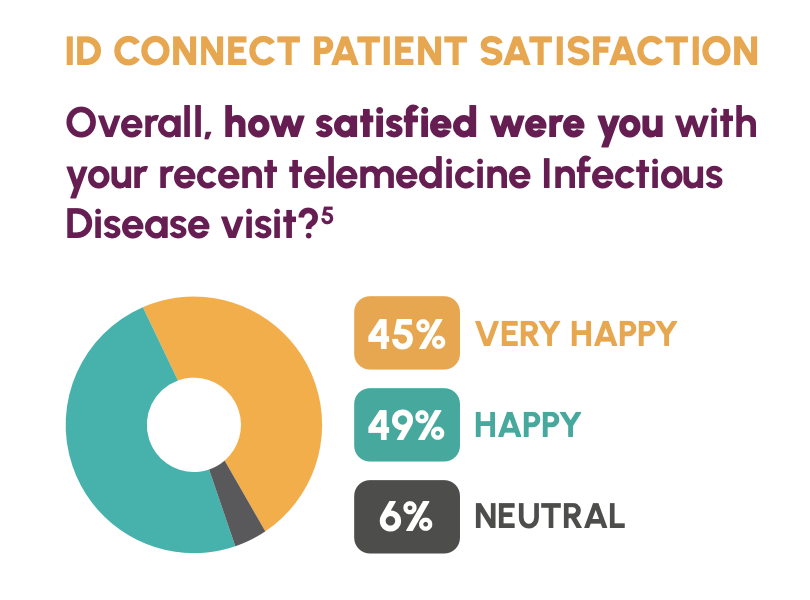
Recent surveys conducted by Infectious Disease Connect with patients and healthcare providers using and experiencing their tele-ID services indicate nearly universal acceptance and high degrees of satisfaction. On questions such as overall satisfaction with telemedicine ID visits, 94% indicated they were “very happy” or “happy” with the experience. 90% rated their comfort level with the tele-presenter nurse assisting with the exam as “very happy”, while 95% of respondents indicated they would be willing to use inpatient telemedicine care again in the future.
On the provider side, two recent experiences sum up the benefits.
“Since we started using ID Connect’s telemedicine consultation service, we’ve had no complaints from patients who have been comfortable with the experience. What’s more important to patients is who the information about their care comes from, not how they receive that information.”
Elizabeth Piccione, M.D., president of UPMC Jameson and UPMC Horizon
While a Director of Telemedicine with another healthcare organization commented, “Without your service, we would need to transfer 40% to 50% of our patients with infections to tertiary facilities. We admire ID Connect’s commitment to follow-up, as well as its robust documentation in the EMR. We never feel like we have to get on a call because the ID specialist can handle it.”
Telemedicine is a Viable Option – And It Is Only Getting Better

As telemedicine continues to expand and become a widely accepted – and often preferred – form of care, patients and physicians are learning how incorporate tele-specialists to improve the quality of care. The ever-growing ID shortage, physician burnout and attrition, and ongoing threat of serious infectious disease complications and antimicrobial resistance are real challenges that require a dependable solution. The convenience and resources of tele-ID ensures hospitals are well equipped to manage and treat both complex and everyday infectious disease cases with care and integrity.
Contact sales@idctelemed.com to learn more and start a conversation about your hospital or healthcare system’s ID needs and goals for the future.
References and Data Sources
- Walensky RP, McQuillen DP, Shahbazi S, Goodson JD. Where Is the ID in COVID-19? Ann Intern Med. 2020 Oct 6; 173(7): 587-589.
- Gupta N, Bariola RJ, Mellors JW, Abdel-Massih RC. In-Person Versus Tele-Infectious Disease (Tele-ID) Care: Is One Better? Open Forum Infect Dis. 2022; 9(8): Ofac410.
You might also like…

Infectious Disease Connect Strengthens Clinical, Operational, and Growth Leadership Amid Continued Expansion

The Hidden Risks of Limited Infectious Diseases Coverage
80% of U.S. Counties Lack ID Coverage. Telemedicine Is Helping Close the Gap.