


This poster highlighting tele-ID consults was originally presented at IDWeek 2021, held Oct. 19-23 in Washington, D.C.
Aryn Andrzejewski, M.D.1; Rima C. Abdel-Massih, M.D.2,3; John W. Mellors. M.D.2; Nupur Gupta, DO MPH2
1Division of General Internal Medicine, University of Pittsburgh Medical Center; 2Division of Infectious Disease, University of Pittsburgh Medical Center; 3Infectious Disease Connect, Inc.
Contact: guptan8@upmc.edu
Conclusions
- Tele-ID is an effective alternative to in-person ID care at academic medical centers.
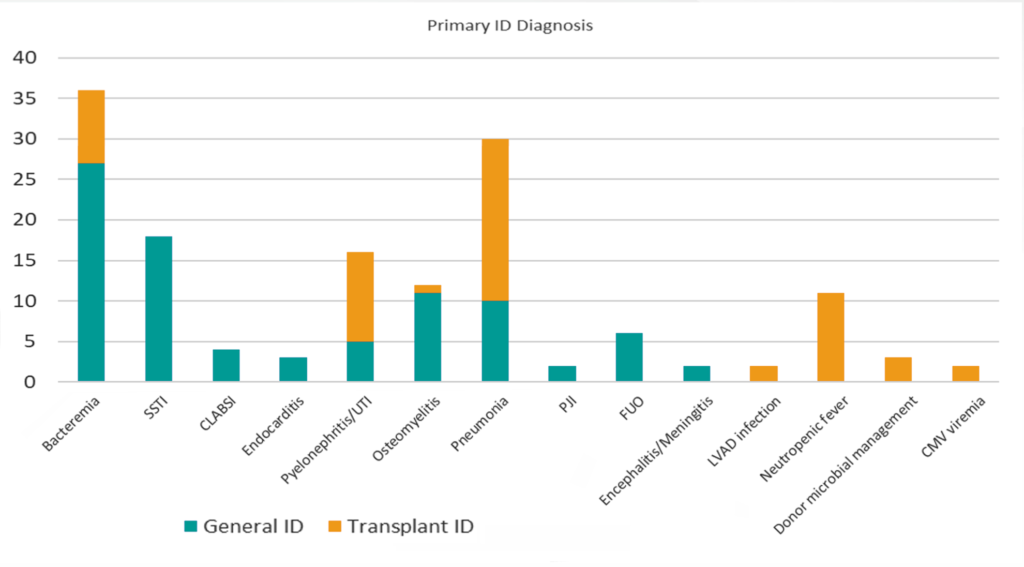
- General ID and Transplant ID services were able to evaluate a large proportion of patients with varied ID diagnosis using telemedicine at the onset of the pandemic.
- Amongst the cases, hospital LOS, 30-day mortality and 30-day readmissions were low.
- Compared to matched in-person controls, tele-ID demonstrated significantly lower 30-day readmission and shorter ICU LOS.
Background
- Inpatient tele-ID consults are effective at community hospitals.
- Tele-ID is not utilized at academic medical centers (AMCs) because of the availability of ID physicians in urban settings.
- During the COVID-19 pandemic, tele-ID was implemented at AMCs to minimize exposure and conserve personal protective equipment.
Questions Addressed
- What are the outcomes for patients seen via tele-ID at AMCs?
- Is there a difference in outcomes for patients seen via tele-ID compared to in-person ID care at AMCs?
- Can a tele-ID service make complex diagnoses compared to an in-person service?
Methods
- Longitudinal, matched, case-control study
- Study Sites:
- 3 tertiary AMCs in Pittsburgh, PA
- Over 1,300 beds
- Cases: Tele-ID consults
- March 1, 2020 – May 31, 2020
- Evaluated via video, electronic consults, inpatient phone calls
- Controls: In-person consults
- March 1, 2019 – November 30, 2019
- Evaluated via in-person only prior to the pandemic
- Matched by demographics and ID diagnosis
- Both groups evaluated by existing general ID or transplant ID physicians in the UPMC ID Division
- COVID-19 diagnosis excluded
Characteristic of the Tele-ID Cases (3/1/20 – 5/31/20)
| General ID | Transplant ID | |
|---|---|---|
| Number of consults | 125 | 81 |
| Initial consult location – Floor (#) | 111 | 61 |
| Average age (years; range) | 57.8 (20-92) | 56.8 (24-85) |
| Female (%) | 52 (42%) | 39 (48%) |
| Caucasian (%) | 92 (64%) | 64 (79%) |
| Average Charlson Comorbidity Index (range) | 3.2 (0-13) | 4.4 (0-11) |
| Heart transplant (#) | 9 | |
| Lung transplant (#) | 9 | |
| Kidney transplant (#) | 18 | |
| Stem cell transplant (#) | 4 | |
| CAR-T (#) | 2 | |
| Liver transplant (#) | 12 | |
| Multiple transplants (#) | 7 | |
| Pre-transplant evaluation including LVAD (#) | 18 |
Characteristic of the Tele-ID Cases (3/1/20 – 5/31/20)
| General ID | ||
|---|---|---|
| Average Hospital LOS post-ID consult (days; range) | 6.26 (-0.11 – 39.9) | 6.5 (0.08-33.8) |
| Average ICU LOS (days; range) | 12 (0-27) | 7.6 (0-33) |
| In-hospital mortality (%) | 5 (4%) | 3 (3.7%) |
| 30-day mortality (%) | 3 (2.4%) | 5 (6.2%) |
| 30-day readmission for 1o ID infection (%) | 7 (5%) | 10 (12%) |
Primary Outcomes of Matched In-Person Controls to Tele-ID Cases
| Controls | Cases | Standardized Differences | 95% CI | p-value | |
|---|---|---|---|---|---|
| Number | 633 | 65 | |||
| In-hospital mortality | 7.7% | 4.0% | 0.156 | -12.8 to 1.9% | 0.143 |
| 30-day mortality | 9.8% | 4.9% | 0.187 | -15.6 to 0.9% | 0.080 |
| 60-day mortality | 12.9% | 8.6% | 0.139 | -15.2 to 2.4% | 0.155 |
| 30-day readmission | 17.3% | 5.1% | 0.394 | -25.0 to -4.9% | 0.004 |
| ICU admission | 53.8% | 46.6% | 0.145 | -16.7 to 10.6% | 0.665 |
| ICU LOS (hours) | 269.2 | 118.1 | 0.545 | -365.5 to 81.7% | 0.002 |
Broad Range of ID Diagnosis via Telemedicine
You might also like…

Infectious Disease Connect Strengthens Clinical, Operational, and Growth Leadership Amid Continued Expansion

The Hidden Risks of Limited Infectious Diseases Coverage
80% of U.S. Counties Lack ID Coverage. Telemedicine Is Helping Close the Gap.